I know some of you want me to just “Stick to weather!” but I just can’t. Not in good conscience. I can’t just sit here and watch people get sick and die without trying to help. And the only way I know how to help to to try and put everything that is happening into better context.
Is everything as bad as it seems? Probably not.
Is everything better than it seems? Probably not.
Is everything just fine? Absolutely not.
Here are the latest numbers for Mississippi. This is a squeezed-down image, but click on it will reveal the entire thing full-sized.

And here is what the numbers in Mississippi look like, graphically, since this all started.
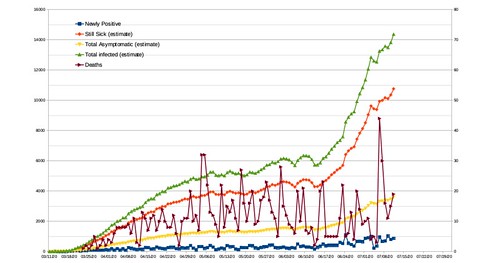
The numbers continue to rise. And not just because “there are more tests” but because there are literally more people infected.
Fewer thermometers doesn’t make it cooler, it just means we have a less accurate representation of what the general temperature over a given area is.
Going-going, back-back, to science-science
I know it has been a long time since many of you have sat in a science classroom. Probably even longer since you’ve sat down and done a science experiment! And that makes sense. A lot of people (except nerds like me) took science in high school, maybe a few classes in college and moved on with life.
But there were some very important lessons in Science Class that may not have fully resonated with some of you when you were younger. So I wanted to quickly revisit them.
Misinformation, misrepresentation
A lot like the multiverse (hypothesis about multiple universes), misinformation seems to bifurcate, or fork into two, frequently. For every piece of real information, someone can come up with two pieces of misinformation explaining it. Then the next person comes up with two pieces of misinformation to explain that.

For example, there is real data to show that COVID-19 spreads differently in different climate. A paper titled, “Temperature, Humidity and Latitude Analysis to Predict Potential Spread and Seasonality for COVID-19” released in mid-March (here is my post about it) showed that in certain warmer climates it wasn’t spreading as quickly and in other cooler climates the spread was more rampant.
The authors made this interpretation: “The distribution of significant community outbreaks along restricted latitude, temperature, and humidity are consistent with the behavior of a seasonal respiratory virus. Additionally, we have proposed a simplified model that shows a zone at increased risk for COVID-19 spread. Using weather modeling, it may be possible to predict the regions most likely to be at higher risk of significant community spread of COVID-19 in the upcoming weeks, allowing for concentration of public health efforts on surveillance and containment.”

Shortly after this paper came out, many people started to make claims that “The virus doesn’t like heat” and that “when it warms up, the virus will just die out.”
And you may say, “well that seems like a reasonable conclusion, Nick.”
But, sadly, it is not.
That is not what the paper’s authors were suggesting. Just because, at that point, the spread was higher in areas with a certain climate does not mean that the virus will “die” in areas where the climate is different. It simply showed that a certain climate was allowing for a higher risk of community spread. Why? The authors did not elaborate. That wasn’t the purpose of the study. The purpose of the study was only to identify where and find a possible connection.
This was a time when real data – and even an interpretation of that data by scientists – was then used by those spreading misinformation.
So now when case numbers increase in areas where the climate does not match those original findings, people rebuke the numbers or rebuke the science. In places like Mississippi, Alabama, Florida, Texas and Arizona, an increased number of new cases is met with “they got the science wrong, it was supposed to die” or “I don’t think the numbers are going up because it is too hot. The media is lying to us, the virus dies in the heat.”
Both of those statements are not fact. Those statements are fiction. The science got it right, the authors identified the areas where community spread was the fastest and those areas shared a common climate. The authors made a predicting that places like New York could be next. But that was it. That was the end of the science.
The problem wasn’t the science. The problem was non-scientists spreading misinformation, misrepresenting what the science found.
Opening schools and dealing with “What is a fact?”
I think most of you do more science on a regular basis than you may realize.
If a friend across town called you up right now and said, “I looked out my window and the sky is green.” and you looked outside and the sky was the normal blue color, you would may ask the person to take a picture or somehow prove the sky was green.
Maybe they take a picture and send it over and sure enough it was green. You look outside again, and it is still blue. So you may ask the person if they changed the picture in any way. Or if the window they were looking out of was dirty. You would try to remove all doubt possible from the observation your friend was making.
You probably remember that science has found that repeated study of the sky shows that blue is the actual color. That has been found through observations across multiple different observers as well as through experimentation in the lab looking at the chemical properties of the atmosphere and how it interacts with light.
So you would do all that you could to make sure it was actually green, like your friend was suggesting.
That science! And that is how science finds facts!
Merriam-Webster defines a fact as “a piece of information presented as having objective reality.” And the objective part is important. It is something that can be repeatedly observed by multiple different people. This becomes especially with COVID-19.
In my example with the green sky, it is easy to “check” if the claim your friend is making is true… just look outside.
But with COVID-19, it isn’t as easy. When someone claims that “Kids don’t get sick from COVID-19” you can’t just look out your window to verify if that is true. Further more what does “get sick” mean? Does the person mean that kids don’t show symptoms? Or that kids aren’t hospitalized? Or that kids never get infected at all?
Data show that the death rate is lower for humans under the age of 18. Data show that the hospitalization rate is lower for humans under the age of 18.
One observation may be that “Kids don’t get sick from COVID-19” but that observation is incomplete.
There is no data to show children, when in contact with the virus, are being infected at a rate any differently than any other age group. The data only show that the number of hospitalizations and deaths are lower from COVID-19 than people that are older.
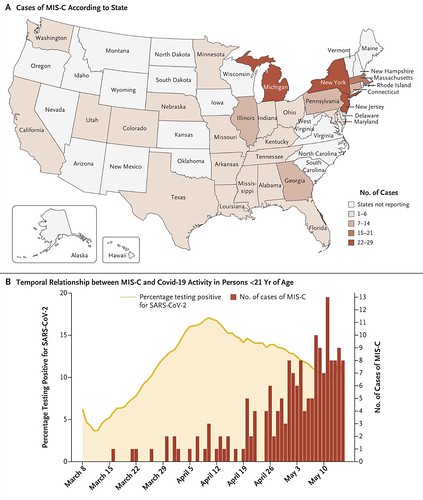
From here there are two two concerns. If there is no data to support that children cannot carry the virus, we must assume that they can carry the virus, and thus transmit it to others. And, the medical community has seen a rise in the number of MIS-C cases resulting from a prior COVID-19 infection in children.
From the Mayo Clinic:
Multisystem inflammatory syndrome in children (MIS-C) is a serious condition in which some parts of the body — such as the heart, blood vessels, kidneys, digestive system, brain, skin or eyes — become inflamed. Inflammation typically includes swelling, often with redness and pain.
Many, but not all, children with MIS-C test negative for a current infection with the virus that causes COVID-19. Yet evidence indicates that many of these children were infected with the COVID-19 virus in the past, as shown by positive antibody test results.
An antibody test with a positive result means that the child’s immune system developed blood proteins (antibodies) that fought the COVID-19 virus. Sometime this blood test is the only indication that the child was ever infected — meaning the child may have fought the infection without ever having shown signs or symptoms of COVID-19. Still, some children with MIS-C are currently infected with the virus, usually confirmed by detection of the virus on a swab taken from the back of the nose or throat.
From the New England Journal of Medicine:
We report on 186 patients with MIS-C in 26 states.
The median age was 8.3 years,
115 patients (62%) were male, 135 (73%) had previously been healthy,
131 (70%) were positive for SARS-CoV-2 by RT-PCR or antibody testing,
164 (88%) were hospitalized after April 16, 2020.
Organ-system involvement included..
Gastrointestinal system in 171 patients (92%)
Cardiovascular in 149 (80%)
Hematologic in 142 (76%)
Mucocutaneous in 137 (74%)
Respiratory in 131 (70%).
The median duration of hospitalization was 7 days (interquartile range, 4 to 10);
148 patients (80%) received intensive care,
37 (20%) received mechanical ventilation,
90 (48%) received vasoactive support,
4 (2%) died.
Coronary-artery aneurysms (z scores ≥2.5) were documented in 15 patients (8%)
Kawasaki’s disease–like features were documented in 74 (40%)
Most patients (171 [92%]) had elevations in at least four biomarkers indicating inflammation.
The use of immunomodulating therapies was common:
intravenous immune globulin was used in 144 (77%),
glucocorticoids in 91 (49%),
interleukin-6 or 1RA inhibitors in 38 (20%).
It appears from the NEJM study that MIS-C is pretty potent to children. While the numbers of MIS-C are very low, the research for this illness is still only beginning. And some of the first numbers show that the change from COVID-19 infected to MIS-C symptoms can be as many as four to eight weeks. So if your child is infected today, MIS-C symptoms may not show up until August or September.
This complicates the idea that “Kids don’t get sick from COVID-19” because research has found that MIS-C is directly related to a COVID-19 infection in 70-percent of the cases today date. And 88-percent of the total cases of known MIS-C ended up in hospitalization.
So, simply saying, “Kids don’t get sick from COVID-19” is not a fact. Nor is there evidence to support such a claim. Even saying “the death rate for kids isn’t as high from COVID-19” may not be accurate. That’s not to say it is definitely inaccurate. But science just doesn’t know yet due to the lag time between a COVID-19 infection and the on-set of MIS-C.
Evidence for COVID-19 fraud
A lot of posts have been circulating social media with claims of COVID-19 fraud. I won’t link to any of them, but I’m sure you’ve seen them.
The problem is that “evidence” in this case is often second-hand accounts posted without proof, Things like, “My brother is a doctor and says positive COVID-19 tests are being double-counted at the labs on purpose.” or “My aunt is a nurse and sent in 10 empty vials and five came back COVID-19 positive.”
The problem is there is no physical documentation of these things actually occurring. No videos of empty vials being tagged and packaged only to have the same tags come back positive days later. There are no pictures of documents showing tests being double-counted.
Going back to the Merriam-Webster dictionary, evidence is “the available body of facts or information indicating whether a belief or proposition is true or valid.”
And in this case, there is no “evidence” brought forward with the claims. Instead, this is simply conjecture. Which is an opinion or conclusion formed on the basis of incomplete information.
The few videos that are circulating showing “nurses going undercover to expose the truth,” when viewed objectively, are mostly suspect with questionable video, limited examples, and incomplete frames of reference. For example, in these videos the name of the hospitals aren’t given and the name of the offending doctors and nurses aren’t given. Seems odd that a person would go through all of the trouble to prove something was happening, and then leave the people responsible for the wrong-doing out of it.
Imagine if someone video’d “a bank robbery” and gave it to the police. The video showed the teller handing 50,000 dollars to a person with their hands in their pockets, holding what looked like a gun, and then the person ran out the door.
The person with this video gave it to the police and said, “I am going to show you this video of people robbing a bank, but I will not name the people or the bank that was robbed.”
That would be odd. There would be a lot of incomplete information.
Again, evidence is based on facts. And facts are things that are objectively verifiable and reproducible by others. If one post or one video shows something that is – even slightly – questionable and it can’t be reproduced by others or supported by other data, then it isn’t fact. And it can’t be called evidence.
And there isn’t any evidence that COVID-19 testing fraud is occurring. So when you see those posts and think, “Yeah that is making a really good point!”
Perhaps it is. But what is the evidence? Is there any? And is it real evidence, or just second-hand conjecture?
The Bottom Line
My whole goal here is to help everyone recognize real information and misinformation. Because the level of misinformation is only increasing. In fact, if you look back to that first example. You can imagine that “misinformation” continue to double while the size and number of the actual data remains the same. It means that soon the amount of misinformation will out-number the actual real information by more than 100-to-1 in about seven steps.
This is a huge problem when you are “under informed” about something. Because the amount of misinformation you have access to vastly out-numbers the amount of actual real information you have access to.
And don’t let the term “under informed” make you feel weird. It is just a way to explain a topic that you are unfamiliar with. For example, I am “under informed” about plumbing. If someone tells me something that “seems” right, I will likely have to research it to make sure it’s right. I can’t just simply agree or refute a claim.
When it comes to COVID-19 it is good to listen to the state health departments. You can listen to the doctors in the medical community, doctors in the medical research community, and doctors with the CDC and doctors with the WHO. Because it is their job to get it right. And to purposefully allow themselves to be incorrect would not be advantageous to their career path.
On the flip side of things, when SuperCOVIDFacts2020 facebook page claims that there is a video from an undisclosed location with a doctor in 95-degree heat putting watermelon on a swab then pointing at a computer screen that reads “COVID POSITIVE” claiming that this is the reason it is safe for kids to be in school because they can’t get sick… you know that you may want to think about investigating those claims.
Before you go…
I know this may feel very doom and gloom. I’m not trying to “get you down” or “scare you” about this stuff. But if you to see things for what they really are, and that makes to a little anxious, that’s okay. You aren’t alone. Many people within the scientific community feel that way. Because there are many unknowns, and the knowns that we do have access to are not great.
But a vaccine is in the works and some of the best medical minds in the world are working hard toward finding a way to beat this thing.


Thank you, Nick. I appreciate a source of reliable information on Covid19.
Keep up the good work.
stick to weather man!!! You are NOT a Doctor you know. Go back to med school for you want to be a doctor. Wished you would leave Mississippi. We don’t need you here.